


서 론
연구의 필요성
환자안전에 대한 중요성은 의료환경이 점차 전문화되고 복잡해지면서 더욱 강조되고 있다[1]. 환자안전은 의료의 기본 원칙이며 의료의 질을 결정하는 주요한 구성요소로, 우리나라는 2016년 환자안전법을 시행하여 환자안전을 정책적으로 강화하고 있다[2]. 그러나 보건복지부 통계에 따르면 2017년에 비해 2021년의 환자안전사고 발생률은 3배 이상 증가하였으며, 그에 따른 사망률도 약 3배 증가하고 있다[3]. 또한 세계보건기구(World Health Organization)는 환자안전사고에 대해 전 세계적인 질병 부담의 14번째 주요 원인으로 보고하고 있으며[4], 환자안전사고는 국외 환자 사망률의 9.5%로 환자 사망원인 3위를 차지하고 있다[5].
Joint Commission [6,7]에 따르면, 환자안전사고의 적신호사건에서 약 60%가 의사소통의 오류로 인해 발생되며, 임상판단과 의사결정의 오류도 주요 원인으로 보고되고 있다[6]. 의료인과 환자 사이의 의사소통은 치료적 관계 확립과 양질의 의료서비스에 필수적이며[8], 전문직 간의 원활한 의사소통은 의료오류를 감소시키고 질적인 의료 서비스 제공에 있어 중요한 요인이다[9]. 특히 간호사는 다양한 의료 전문인들과 환자, 보호자 사이에서 중재자 역할을 하기 때문에 간호사의 의사소통은 간호의 질과 환자의 안전을 증진시키는 데 보다 중요한 요인으로 작용하게 된다[10].
또한, 임상판단은 대상자의 특정 상황에 요구되는 적절한 중재를 하기 위한 의사결정 과정으로 정의되며, 의사결정과 유의어로 사용되고 있다[11,12]. 복잡하고 때로는 긴박한 임상현장에서 간호사의 신속하고 정확한 임상판단은 환자안전과 직접적으로 연결되는데[13], 이는 간호사의 잘못된 임상판단이 환자의 상태 악화와 같은 중요한 정보를 감지할 수 없게 하고 부정적인 결과로 초래할 수 있기 때문이다[14]. 따라서, 교육 및 임상현장에서 간호대학생과 간호사의 의사소통과 임상판단능력을 향상시키기 위한 교육은 필수적이라고 할 수 있다.
이를 반영하여 한국간호교육평가원은 4주기 간호교육인증평가의 학습성과 중 하나로 안전과 질 향상 원리를 적용하고 건강증진과 건강문제 해결을 위해 보건의료팀과 협력하는 것을 설정하였다[15]. 이에 따라 각 간호대학에서는 학생들의 의사소통 및 임상판단능력을 향상시키기 위해 다양한 방법을 활용하고 있는데, 최근 들어 시뮬레이션을 이용한 교육이 증가하고 있다. 시뮬레이션 교육은 실제와 유사한 현실을 구조적으로 재현하여 학습자로 하여금 생생하게 현실을 경험하게 하는 것으로[16], 임상술기뿐만 아니라 비판적 사고를 통한 임상판단, 의사결정, 의사소통, 협동능력을 강화하는 데 효과적인 것으로 보고되고 있다[17,18]. 또한 임상현장실습 시 직접 환자를 상대하는 것이 점점 어려워지고 있는 현실에서[16], 시뮬레이션 교육은 안전한 환경에서 학습자가 독립적으로 의사결정 및 임상적 판단을 내리는 연습을 할 수 있는 장점이 있다[16,19]. 따라서, 의사소통과 임상판단을 향상시키기 위해 간호대학생과 간호사에게 시행되고 있는 시뮬레이션 교육의 효과를 파악하는 것은 향후 교육 프로그램 개발을 위해 필수적이다.
지금까지 의사소통과 임상판단능력을 향상시키기 위한 시뮬레이션 교육 중재연구는 활발하게 이루어지고 있으나 이러한 교육중재의 효과를 체계적으로 검토하여 통합적인 결론을 얻기 위한 메타분석 연구는 미비하였다. 시뮬레이션 교육의 의사소통과 임상판단능력의 효과를 분석한 메타분석 연구를 살펴보면, Lee [20]의 연구에서는 임상판단능력은 효과가 큰 것으로 나타났으나 의사소통은 통계적 유의성 없는 것으로 나타난 반면, Kim과 Ham [21]의 연구에서는 의사소통과 임상판단능력의 효과가 큰 것으로 나타났다. Lee [20]의 연구는 2014년 2월까지 시행된 국내·외 간호대학생만을 대상으로 한 연구를 포함하였고, Kim과 Ham [21]의 연구는 2000년부터 2014년까지 시행된 간호사와 간호대학생을 대상으로 한 국내 연구만 포함하여 한계가 있었다. 또한, 기존의 메타분석 연구에서는 시뮬레이션 교육 후 지식이나 만족도, 자신감, 자기효능감, 임상수행능력, 문제해결능력 등에 중점을 두어 분석하여[22,23] 연구 설계에 대한 부분을 파악하는 것에는 제한이 있었다.
이에 본 연구에서는 국내·외 문헌으로 2010년부터 2022년 6월 21일까지 발표된 간호대학생과 간호사를 대상으로 한 시뮬레이션 교육이 의사소통 및 임상판단능력에 미치는 효과를 검증한 실험연구들을 체계적으로 고찰하고, 연구 결과를 종합하는 메타분석을 시도하고자 한다. 또한 의사소통 및 임상판단능력 향상을 위한 시뮬레이션 교육 설계 따른 효과를 분석하여, 간호의 질과 환자안전 증진을 위한 의사소통과 임상판단능력을 증진시킬 수 있는 시뮬레이션 교육 프로그램 개발의 기초 자료와 후속 연구에 대한 방향성을 제시하고자 한다.
연구 방법
연구 설계
본 연구는 시뮬레이션 교육이 간호대학생과 간호사의 의사소통, 임상판단능력에 미치는 효과를 파악하기 위해 무작위 대조군 및 비무작위 대조군 실험연구를 선정하여 관련된 변수에 대하여 체계적 문헌고찰과 메타분석을 시행한 연구이다.
문헌 선정 기준 및 배제 기준
본 연구는 간호대학생과 간호사에게 시뮬레이션 교육이 미치는 효과를 파악하기 위해 Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) 그룹이 제시한 체계적 문헌고찰 보고 지침에 따라 수행되었다. 체계적 문헌고찰의 자료선정은 핵심질문 participants, intervention, comparisons, outcomes, study-design (PICO-SD)을 통해 국내·외 데이터베이스를 검색한 후 선정 및 배제 기준에 부합하는 연구를 선정하였다.
문헌 검색과 선정
본 연구는 체계적 문헌고찰의 체계적 검색방식을 활용하여 선행연구자료 검색을 진행하였다. 선정한 핵심질문은 시뮬레이션을 적용한 간호교육의 효과이다. 선행연구자료 검색을 위해 선정한 PICO-SD 중 P AND I의 검색전략을 선정하였고, 민감도 높은 검색을 진행하였다. 데이터베이스는 COre, Standard, Ideal (COSI) 모델 이론에 따라 적합한 데이터베이스를 탐색하였고, 그 중 간호학에서 주로 사용되는 PubMed (https://pubmed.ncbi.nlm.nih.gov/), EMBASE (https://www.embase.com/), Cochrane Library (https://www.cochranelibrary.com/), CINAHL (https://search.ebscohost.com/)을 해외 데이터베이스로 선정하였다. 국내 데이터베이스로는 국내에서 가장 많이 활용되는 RISS (https://www.riss.kr/index.do)와 KISS (https://kiss.kstudy.com/index.asp)를 선정하였다.
방법론에 입각한 체계적 선행연구자료검색을 위한 검색어는 PubMed, Cochrane Library에서는 MeSH 용어를 활용하였고, EMBASE에서는 Emtree 용어, CINAHL에서는 CINAHL Headings를 활용하였으며, 국내 데이터베이스인 RISS, KISS의 경우 주 키워드로 조합하여 활용하였다. 또한 관련된 자연어를 추가하였고, 검색어간 불리언 연산자(AND, OR, NOT)를 조합하여 검색식으로 변환 후 검색하였다. 간호사, 간호대학생은 “Nurses”, “Students, Nursing”, “Education, Nursing”의 MeSH 용어와, “nurse”, “nursing student”, “nursing education”의 Emtree 용어를 검색어로 선정하였다. 시뮬레이션 교육은 “Simulation Training”, “Patient Simulation”의 MeSH 용어와 “simulation training”, “patient simulation”의 Emtree 용어를 검색어로 선정하였다(Appendix 1).
2022년 6월 21일부터 일주일간 검색을 진행하였으며, 체계적 문헌고찰 지침인 PRISMA의 흐름도에 근거하여 연구 문헌을 선정하였다. 먼저, 데이터베이스를 통해 문헌을 검색하였으며 서지 관리 프로그램(EndNote; Clarivate Analytics, Philadelphia, PA, USA)을 이용하여 중복문헌을 제거하였다. 이후 제목과 초록을 중심으로 검토하여 본 연구의 선정 기준에 부합하는 문헌을 1차 선정하였다. 선정된 문헌은 전문을 검토하여 최종문헌을 선정하였다. 자료의 수집과 선별은 두 명의 연구자가 독립적으로 수행하였으며, 서로 다른 의견이 있는 경우 연구자간 합의를 통해 결정하였다.
자료 분석
● 분석 대상 연구의 일반적 특성과 방법론적 질 평가
분석 대상 연구의 일반적 특성은 문헌의 저자, 출판연도, 연구 설계, 연구 대상, 중재 유형 및 내용, 결과변수, 측정도구, 결과 및 통계치를 표로 분석하였다. 방법론적 질 평가는 무작위 대조군 연구의 경우 revised Cochrane risk of bias tool for randomized trials (RoB 2.0)와 비무작위 대조군 연구의 경우 a tool for assessing risk of bias in non-randomized studies of interventions (ROBINS-I)를 이용하였다. RoB 2.0은 5개의 영역으로 무작위 배정 과정, 의도한 중재에서 이탈, 중재결과 자료의 결측, 중재결과 측정, 보고된 연구 결과 선택의 비뚤림으로 구성되어 있다. 각 영역의 신호 질문에 대한 응답을 맵핑하는 알고리즘에 따라 평가하였으며 비뚤림의 판단은 낮은 위험, 일부 우려, 높은 위험의 세 가지로 판단한다. ROBINS-I는 7개의 영역으로 교란, 연구 대상자 선택, 중재 분류, 의도한 중재에서 이탈, 자료의 결측, 중재결과 측정, 보고된 연구 결과 선택의 비뚤림으로 구성되어 있다. 각 영역의 비뚤림 위험 판단은 낮음, 중등도, 높음, 매우 높음, 정보 없음으로 판단한다. 이는 연구자 2인이 독립적으로 질 평가를 수행하였으며, 연구자 간의 평가가 일치되지 않는 경우에는 논의를 통해 일치된 결과를 도출하였다.
● 효과크기와 이질성 분석
시뮬레이션 교육의 효과크기 비교를 위해 R 프로그램의 ‘Meta’ package를 사용하여 메타분석을 시행하였다. 개별연구에서 추출된 시뮬레이션 중재 관련 내용과 의사소통, 임상판단능력과 관련된 결과변수의 값은 실험 처치 후-실험 처치 전의 평균차이 및 표준편차를 이용하였고 각각의 실험결과를 표준화하기 위하여 표준화된 평균차이(standardized mean differences, SMD)를 이용하여 계산하였다. 사전에 선별된 개별연구 간의 연구 대상자, 시뮬레이션 시나리오, 측정도구가 다양하여 이질성이 존재한다고 판단되어 요약 통계량을 결합하기 위해 변량효과 모형(random effects model)을 적용하였다. 분석에 포함된 개별연구의 표본크기 차이가 심할 경우에는 효과크기가 과대 추정되는 경향이 있으므로 이를 보완하기 위해 표준화된 평균차이(Hedge’s g)로 효과 크기를 변환하여 95% 신뢰수준으로 값을 산출하였다. 효과크기 해석은 0.20 이상 0.50 미만인 경우 작은 효과, 0.50 이상 0.80 미만인 경우 중간 효과, 0.80 이상인 경우 큰 효과크기로 해석하였다.
전체 연구의 이질성을 확인하기 위해 Higgin의 I2, Cochrance Q값으로 분석하였다. 이질성 검증은 먼저 forest plot을 통해 시각적으로 개별연구의 효과 값의 방향성과 신뢰구간을 검토하였다. 그리고 Higgin의 I2 통계량으로 이질성을 통계적으로 검정하였다. 효과크기의 이질성을 나타내는 지수 I2은 총 분산에 대한 실제 분산의 비율을 나타내며, I2 값 25%는 이질성이 적고, 50%는 중간 정도, 75% 이상은 이질성이 크다고 판단하였다. 메타분석 시 이질성이 확인되는 경우에는 메타 ANOVA를 시행하였으며, 사후 분석은 Wald-test로 분석하였다.
연구 결과
문헌 선정
데이터베이스 검색결과 총 19,135편의 문헌이 검색되었으며, 이 중 서지관리 프로그램인 EndNote를 통해 중복된 문헌을 제외한 후 12,864편의 문헌을 선정하였다. 이를 대상으로 연구 제목과 초록을 확인하여 연구 대상으로 적합한 170개의 문헌을 선별하였다. 선별된 문헌의 전문을 확인하여 조사연구와 질적연구 등 연구 설계가 맞지 않는 문헌 52편, 간호대학생과 간호사만을 대상으로 하지 않은 문헌 4편, 원문 제공이 되지 않는 문헌 2편, 출판언어가 맞지 않는 문헌 8편, 시뮬레이션 교육과 시뮬레이션 교육을 비교하는 등 중재가 맞지 않는 문헌 25편, 결과 변수가 맞지 않는 문헌 18편, 학위논문 및 포스터 등 회색문헌 25편을 제외하였다. 최종적으로 36편의 문헌이 체계적 문헌고찰을 위한 질 평가 대상문헌으로 선정되었다(Figure 1).
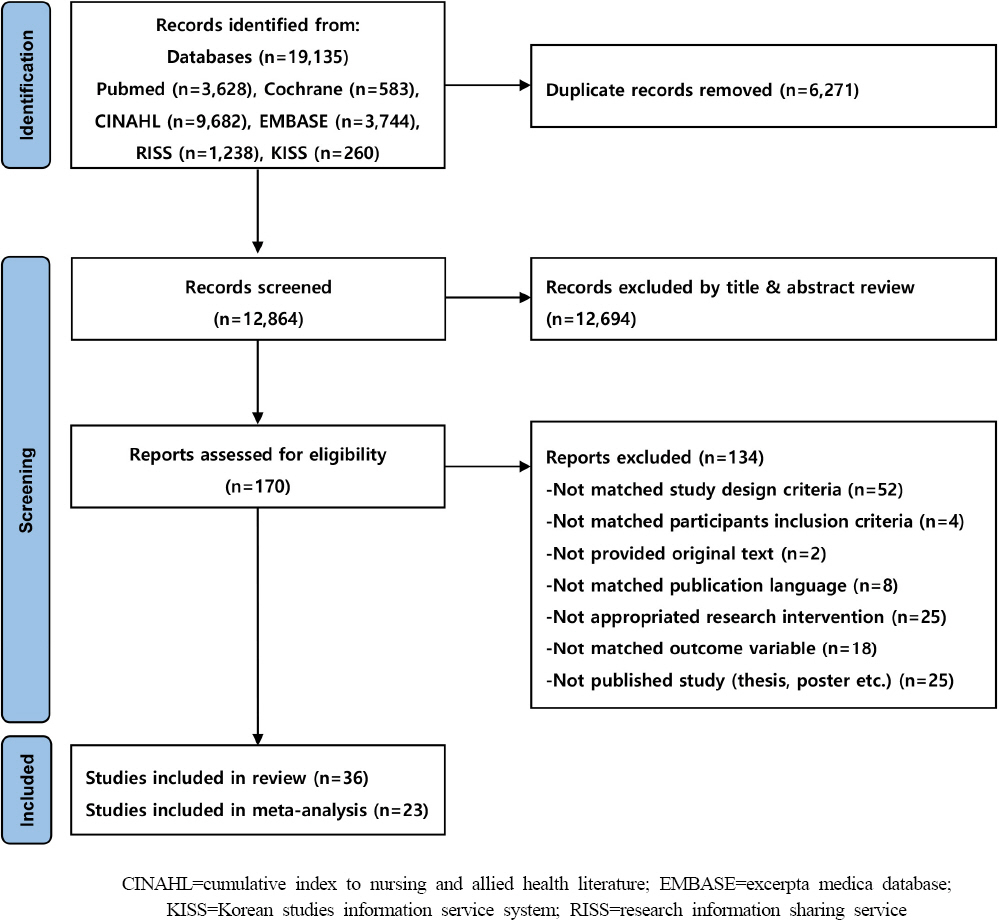
메타분석에 포함된 연구는 체계적 문헌고찰에서 사용된 36편의 문헌 중 결과변수에 대한 사전 측정값이 없는 9편의 연구와 문헌의 질 평가 결과 높은 위험이 있는 4편의 문헌이 제외되어 23편의 연구가 사용되었다.
분석 대상 문헌의 일반적 특성
본 연구에서 선정된 연구 36편의 출판 연도는 2010년부터 2019년까지 출판된 연구 22편, 2020년부터 2022년까지 출판된 연구 14편이었다(Appendix 2). 연구 설계는 무작위대조군 실험연구가 5편, 비무작위 대조군 실험연구가 31편이었으며, 이 중 사전조사를 하지 않은 연구는 9편이었다. 간호사를 대상으로 한 연구는 4편이었으며, 간호대학생을 대상으로 한 연구 32편 중 3학년을 대상으로 한 연구가 15편으로 가장 많았다. 실험군과 대조군의 대상자 수는 최소 14명에서 최대 133명까지 다양하게 나타났으며, 실험군은 평균 44.36명, 대조군은 평균 43.81명이었다.
시뮬레이션 교육 설계 시 이론적 기틀을 사용한 연구는 10편으로, Jeffries의 시뮬레이션 이론을 사용한 연구가 3편으로 가장 많았다. 그 외에는 Kolb의 경험학습이론을 사용한 연구, Jeffries의 시뮬레이션 이론과 의사소통 이론을 함께 사용한 연구, Jeffries의 시뮬레이션 이론과 Kolb의 경험학습이론을 함께 사용한 연구, Peplau의 대인관계모델, 인지부하이론, 의도적 연습, Tanner의 임상판단모델을 사용한 연구가 각각 1편이었다.
시뮬레이션 교육에 사용된 시뮬레이터를 살펴보면, 고충실도 시뮬레이터(high-fidelity simulator)를 사용한 연구는 18편, 표준화 환자를 사용한 연구는 7편이었다. 또한, 팀 기반 시뮬레이션과 같이 시뮬레이터를 사용하지 않는 시뮬레이션 방법을 사용한 연구 4편, 고충실도 시뮬레이터를 포함하여 두 가지 이상의 시뮬레이션 방법을 사용한 연구 2편, 표준화 환자와 애니메이션 시뮬레이션을 활용한 연구 1편, 시뮬레이터에 대해 언급을 하지 않은 연구는 4편이었다.
시뮬레이션 시나리오는 2개 이상 사용한 연구가 16편, 1개를 사용한 연구가 3편, 시나리오 개수에 대한 언급이 없는 연구가 17편이었다. 시뮬레이션 교육 중재기간이 1주 미만인 연구는 1편, 2주에서 최대 15주까지 진행한 연구는 16편이었으며, 나머지 19편의 연구는 시뮬레이션 중재기간에 대하여 언급되어있지 않아 정확한 중재기간을 알 수 없었다.
프리브리핑(pre-briefing)의 구성은 사전학습이나 오리엔테이션만 진행한 경우, 이론 강의만 진행한 경우, 오리엔테이션, 이론 강의 및 실기연습을 모두 진행하는 등 다양하게 이루어졌으며, 이에 따른 시간은 10분에서 최대 2시간까지로 다양하게 나타났다. 시뮬레이션 구동시간에 대해 기술한 연구는 36편 중 28편으로 10분에서 20분간 시뮬레이션을 시행한 연구가 21편으로 가장 많았으며, 7편의 연구에서는 시뮬레이션 시행시간이 30분 이상으로 디브리핑을 포함한 시간을 언급하거나 사전학습과 오리엔테이션을 포함한 전체적인 중재시간을 기술하는 등 정확한 시뮬레이션 시행시간을 알 수 없었다. 디브리핑(debriefing)에 대해 살펴보면, 디브리핑 시간에 대해 언급한 연구는 36편 중 17편으로 10분에서 1시간 이내로 이루어졌으며, 대부분의 연구에서 디브리핑 방법이나 구성에 대해서는 언급되어있지 않아 정확한 내용을 파악할 수 없었다.
분석 대상 문헌의 질 평가
본 연구에서 사용된 문헌의 비뚤림 위험평가는 Figure 2와 같다. 선정된 36편의 연구 중 5편의 무작위 대조군 실험연구는 RoB 2.0을 이용하였으며, 31편의 비무작위 대조군 실험연구는 ROBINS-I를 이용하여 평가하였다(Figure 2) [24-59].
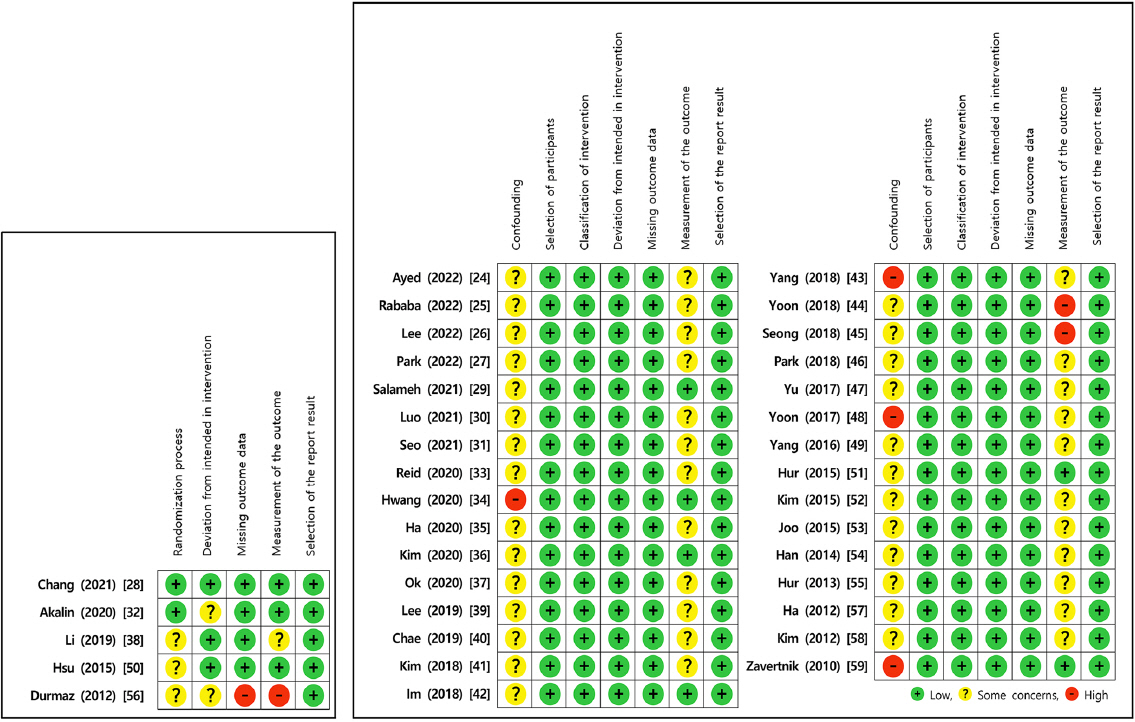
RoB 2.0 도구를 이용한 5편의 질 평가 결과는, 무작위과정에서 2편의 연구에서 낮은 위험도를 보였으며, 3편의 연구에서는 정확한 무작위 과정을 알 수 없었다. 의도한 중재에서 이탈은 3편의 연구에서 낮은 위험도를 보였다. 결측치와 결과측정 부분에서는 1편의 연구에서 높은 위험으로, 해당 연구는 연구 중 데이터 손실과 실험군과 대조군의 상호작용 위험을 보고하였다. 선택적 보고로 인한 비뚤림은 모두 낮은 위험으로 예상되는 대부분의 결과를 보고하고 있었다.
ROBINS-I는 7개의 영역으로 교란, 연구 대상자 선택, 중재 분류, 의도한 중재에서 이탈, 자료의 결측, 중재결과 측정, 보고된 연구 결과 선택의 비뚤림으로 구성되어 있다. 교란은 무작위 배정과 짝짓기 법을 일부 연구에서 사용하고 있었으나 정확한 방법에 대한 기술이 없었으며 대부분의 연구에서 임의배정을 시행하여 27편의 연구에서 중등도 위험을 보였다. 나머지 4편의 연구에서는 대상자를 실험군에 지원을 받거나 실험군과 대조군의 기저상태에 대한 부분을 고려하지 않아 높은 위험도를 보였다. 연구 대상자 선택과 중재 분류, 중재 이탈, 결측치에 대해서는 모든 연구에서 낮은 비뚤림 위험이 측정되었다. 중재 결과 측정은 6편의 연구는 연구자 이외의 평가자가 있으며, 평가자는 대상자가 실험군과 대조군 중 어느 그룹에 해당되는지 알지 못하였고, 평가자간 평가 결과에 영향 미치는 것을 배제하기 위해 각자 다른 시간에 다른 공간에서 독립적으로 동영상을 보면서 평가를 실시하는 등을 보고하여 낮은 위험도로 측정되었다. 반면에 대부분의 연구에서는 자가보고를 하거나 결과 평가자가 연구 대상자가 받는 중재를 알고 있어 중등도의 위험을 나타내었으며, 2편의 연구에서는 중재 전 대상자에게 실험군과 대조군의 중재 내용이 다름을 설명하고 이들이 어느 그룹에 해당되는지 알 수 있어 높은 위험으로 나타났다. 선택적 보고는 모두 낮은 위험으로 계획된 결과를 모두 보고하고 있었다.
전반적 비뚤림 위험은 최소 하나 이상의 높은 위험을 나타낸 7편의 연구는 비뚤림 위험이 높으며, 나머지 연구는 비뚤림 위험이 낮거나 중간으로 분석되었다.
효과크기와 이질성 검정
● 의사소통
메타분석에 포함된 문헌 중 시뮬레이션 교육에 대한 의사소통의 효과를 보고한 연구 20편의 전체 효과크기를 산출하였다. 의사소통의 효과로 의사소통능력을 확인한 연구 15편, 의사소통 명확성을 확인한 연구 2편, 의사소통 자신감, 의사소통 태도 및 의사소통 자기효능감을 확인한 연구 각 1편이 포함되었다. 연구의 이질성 검정 결과 89.9%로 큰 크기의 이질성이 확인되어 변량효과모형을 사용하여 분석하였다. 전체 연구의 효과크기는 0.77 (95% confidence interval, 95% CI=0.43∼1.12, p<.001)로 중간 수준의 효과크기를 보였으며 통계적으로 유의하였다(Figure 3-A).
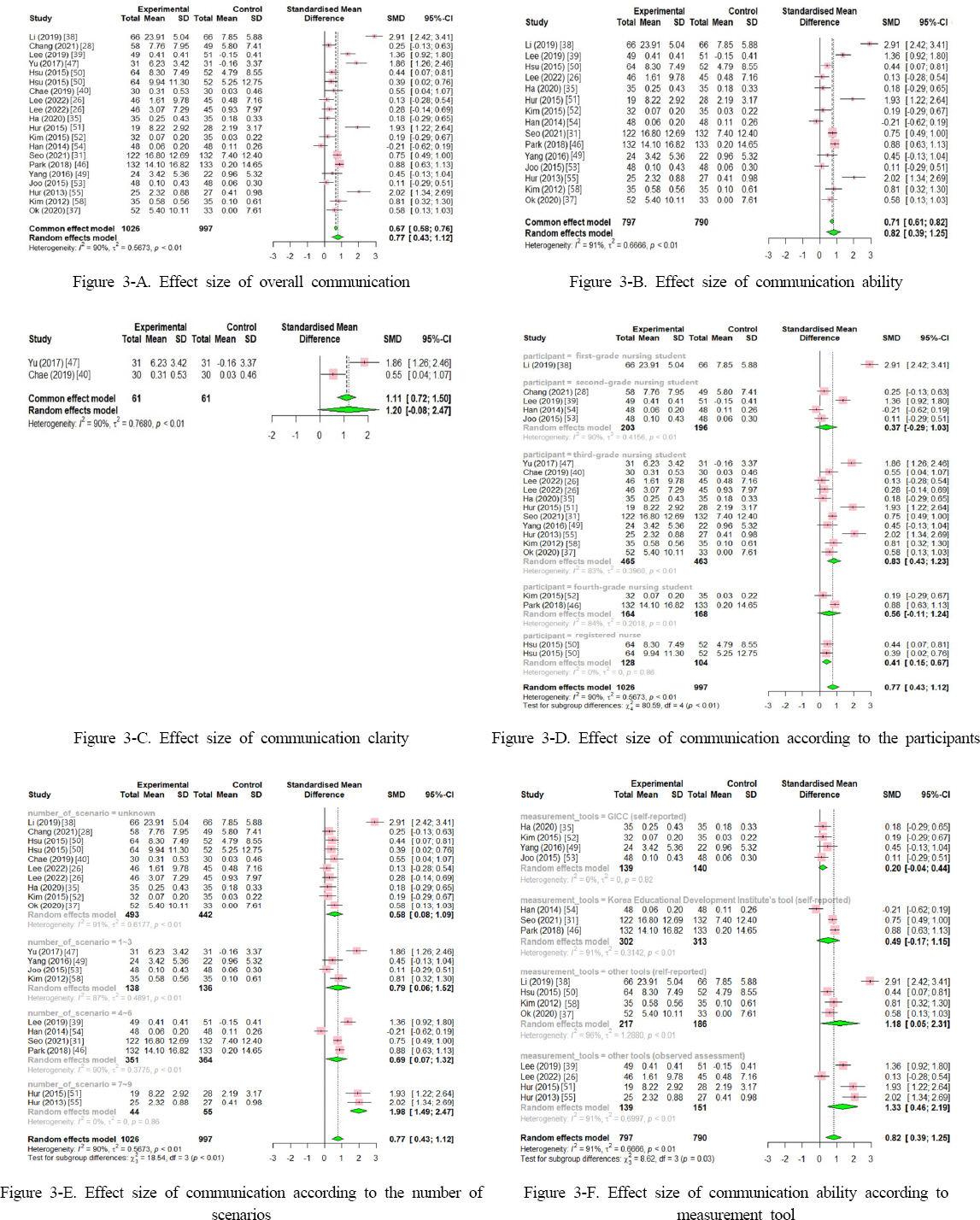
본 연구에서 의사소통의 효과로 의사소통능력을 확인한 15편의 연구의 효과크기를 살펴보면, 연구의 이질성은 검정결과 91.4%로 이질성이 큰 것으로 나타나 변량효과모형을 사용하여 분석하였다. 간호대학생과 간호사를 대상으로 시뮬레이션 교육을 적용하였을 때 의사소통능력에 대한 효과크기는 0.82 (95% CI=0.39∼1.25, p<.001)로 큰 효과크기를 보였으며 통계적으로 유의하였다(Figure 3-B). 또한, 의사소통 명확성을 확인한 2편의 연구를 살펴보면, 연구의 이질성은 검정결과 89.9%로 이질성이 큰 것으로 나타나 변량효과모형을 사용하여 분석하였다, 시뮬레이션 교육을 간호대학생과 간호사에게 적용하였을 때 의사소통 명확성에 대한 효과크기는 1.20 (95% CI=-0.08∼2.47, p<.066)으로 큰 효과크기를 보였으나 통계적으로 유의하지 않았다(Figure 3-C).
시뮬레이션 교육이 간호대학생과 간호사의 의사소통에 미치는 효과에 대한 연구들에서 이질성이 큰 것으로 나타나(I2=89.9%), 이질성에 대한 원인을 분석하기 위해 메타 ANOVA를 이용하여 하위분석을 시행하였다.
∙ 대상자에 따른 효과크기
시뮬레이션 교육 대상자에 따라 1학년, 2학년, 3학년, 4학년, 간호사로 나누어 분석한 결과, 3학년을 대상으로 한 연구의 효과크기가 0.83 (95% CI=0.43∼1.23)으로 큰 효과크기를 보였으며, 집단 간 효과크기 차이는 통계적으로 유의하였다(χ2=80.59, p<.001; Figure 3-D). Wald-test를 통하여 사후분석한 결과 1학년 집단과 그 외 집단 간의 효과크기 차이가 유의하게 나타났다(p<.001).
∙ 시뮬레이션 시나리오에 따른 효과크기
시뮬레이션을 운영은 대부분 하루 또는 1주 간격으로 여러 차례 운영이 되었으며, 교육 시나리오는 1∼9개까지 프로그램에 따라 다양하게 나타났다. 시뮬레이션 교육 프로그램에 사용된 시나리오 개수에 따라 시나리오 개수에 대한 언급이 없는 경우, 1∼3개, 4∼6개, 7∼9개로 나누어 분석한 결과 7∼9개의 시나리오를 운영한 연구의 효과크기가 1.98 (95% CI=1.49∼2.47)로 가장 높게 나타났으며, 집단 간의 효과크기 차이는 통계적으로 유의하였다(χ2=18.54, p<.001; Figure 3-E). Wald-test를 통하여 사후분석한 결과 7∼9개의 시나리오를 사용한 연구와 시나리오 개수를 알 수 없는 경우(p<.001), 7∼9개의 시나리오를 사용한 연구와 1∼3개의 시나리오를 사용한 연구(p=.008), 7∼9개의 시나리오를 사용한 연구와 4∼6개의 시나리오를 사용한 연구 간의(p=.002) 효과크기가 유의하게 나타났다.
∙ 의사소통능력 측정도구에 따른 효과크기
의사소통 명확성을 측정한 2편의 연구에서는 모두 Cho [60]가 수정 보완한 도구가 사용되었으나, 의사소통능력을 측정한 15편의 연구에서는 다양한 측정도구가 사용되었다. 이 중 Global Interpersonal Communication Competence Scale (GICC)을 사용한 연구가 4편으로 가장 많았으며, 한국교육개발원에서 개발한 도구를 사용한 연구가 3편, 자가평가 측정도구가 4편, 관찰평가 측정도구가 4편이었다. 의사소통능력의 효과크기를 분석한 결과, GICC를 사용한 연구의 효과크기가 0.20 (95% CI=-0.04∼0.44)으로 가장 작은 효과크기를 보였으며, 집단 간 효과크기 차이는 통계적으로 유의하였다(χ2=8.62, p=.035) (Figure 3-F). Wald-test를 통하여 사후분석한 결과 GICC와 관찰평가를 한 기타 도구의 효과 크기 차이가 유의하게 나타났다(p<.013).
● 임상판단능력
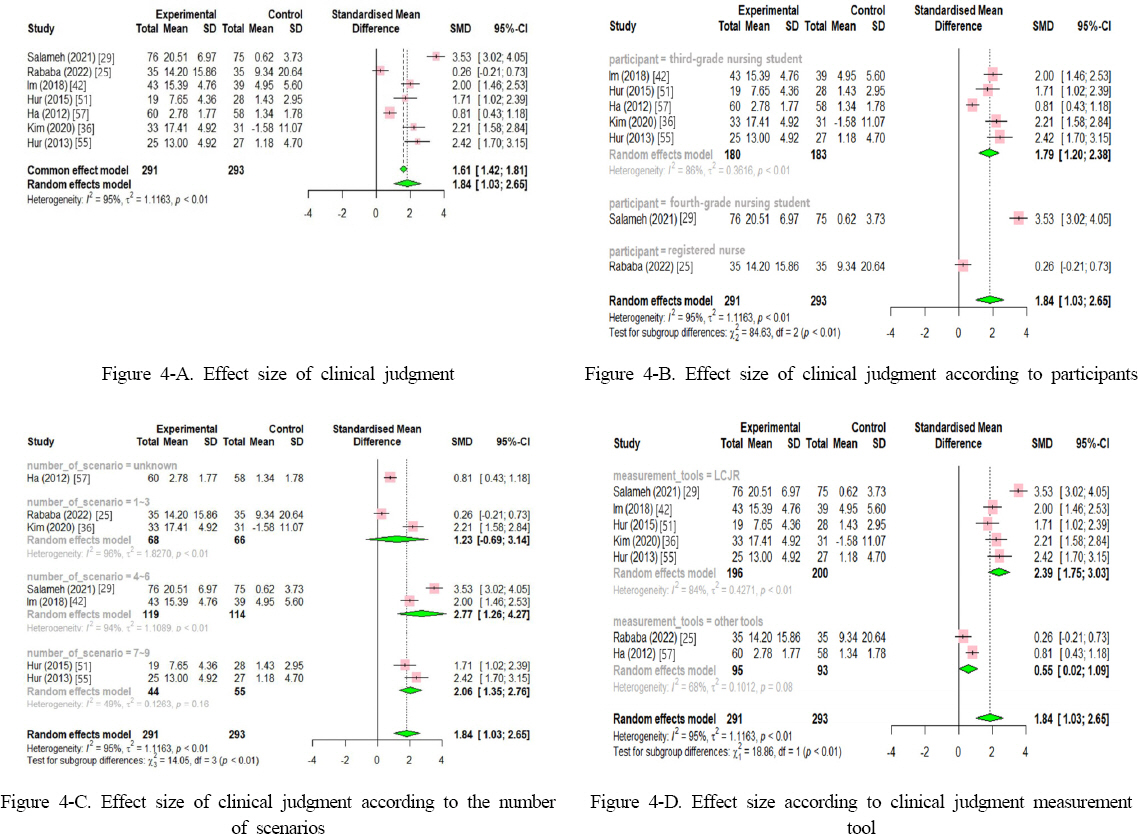
본 연구에서 분석한 연구 중 시뮬레이션 교육에 대한 임상판단능력에 대한 효과를 보고한 7편의 연구에 대한 전체 효과크기를 산출하였다. 연구의 이질성 검정 결과 이질성이 94.7%로 큰 크기의 이질성이 확인되어 변량효과모형을 사용하여 분석하였다. 전체 연구의 효과크기는 1.84 (95% CI=1.03∼2.65, p<.001)로 큰 효과크기를 보였으며 통계적으로 유의하였다(Figure 4-A).
시뮬레이션 교육의 임상판단능력에 대한 효과에 대해 이질성 검정결과 이질성이 큰 것으로 나타나(I2=94.7%), 이질성에 대한 원인을 분석하기 위해 메타 ANOVA를 이용하여 분석을 시행하였다.
∙ 대상자에 따른 효과크기
시뮬레이션 교육 대상자에 따라 3학년, 4학년, 간호사로 나누어 분석한 결과, 3학년을 대상으로 한 연구의 효과크기가 1.79 (95% CI=1.20∼2.38)로 큰 효과크기를 보였으며, 각 집단 간 효과크기 차이는 통계적으로 유의하였다(χ2=84.63, p<.001; Figure 4-B). Wald-test를 통하여 사후분석한 결과 4학년 집단과 그 외 집단 간의 유의한 효과크기 차이를 보였으며(p<.001), 3학년 집단과 간호사 집단에서도 유의한 효과크기 차이가 있는 것으로 나타났다(p<.001).
∙ 시뮬레이션 시나리오에 따른 효과크기
시뮬레이션 교육 프로그램에 사용된 시나리오 개수에 따라 시나리오 개수에 대한 언급이 없는 경우, 1∼3개, 4∼6개, 7∼9개의 시나리오가 사용된 그룹으로 나누어 분석하였다. 그 결과 4∼6개의 시나리오를 운영한 연구의 효과크기가 2.77 (95% CI=1.26∼4.27)로 가장 높게 나타났으며, 집단 간의 효과크기 차이는 통계적으로 유의하였다(χ2=14.05, p<.001; Figure 4-C). Wald-test를 통하여 사후분석한 결과 시나리오 개수에 대하여 알 수 없는 연구와 4∼6개(p=.013), 7∼9개(p=.002)의 시나리오를 사용한 연구 간의 효과크기가 유의하게 나타났다.
∙ 측정도구에 따른 효과크기
임상판단능력을 측정하는 도구에 대해 살펴보면, 7편 중 5편의 연구에서 Laster Clinical Judgment Rubric (LCJR)이 사용되었다. LCJR을 사용한 연구와 그 외 다른 측정도구를 사용한 연구로 나누어 임상판단능력의 효과를 분석한 결과 LCJR을 사용
한 연구의 효과크기는 2.39 (95% CI=1.75∼3.03)로 큰 효과크기를 보였으며, 각 집단 간 효과크기 차이는 통계적으로 유의하였다(χ2=18.86, p<.001; Figure 4-D).
출판편향 검정
메타분석에 포함된 연구에 대한 출판편향을 시각적으로 확인한 결과, Funnel plot이 전반적으로 대칭적인 형태를 보이지 않으며, 일부 연구들이 삼각형 내 존재하지 않으므로 출판편향을 의심할 수 있다. 또한 Egger 회귀분석 방법을 통해 확인한 결과, bias=5.86 (p=.024)으로 출판편향이 존재하는 것으로 확인되었다. 따라서 출판편향 보정을 위해 Trim-and-Fill 방법을 적용하여 추가로 분석하였다. 4편의 연구에 대한 가상의 효과크기를 투입하여 보정한 결과, 시뮬레이션 교육의 효과크기는 0.73 (95% CI=0.29∼1.18, p<.001)으로 나타나 보정 전보다 효과크기에 변화가 있음을 확인할 수 있고 통계적으로 유의하였다(Figure 5).

논 의
본 연구는 간호대학생과 간호사의 시뮬레이션 교육 효과를 파악하기 위해 무작위 대조군 실험연구 및 비무작위 대조군 실험연구를 선정하여 효과를 분석하고, 시뮬레이션 교육 중재 프로그램의 기초자료를 제공하기 위해 체계적 문헌고찰 및 메타분석을 시행한 연구이다.
본 연구의 메타분석에 포함된 시뮬레이션 교육이 간호대학생과 간호사의 전반적인 의사소통에 미치는 효과크기는 0.77로 중간 수준의 효과크기로 나타났다. 그중 의사소통능력을 효과로 보고한 연구가 15편으로 가장 많았고 큰 효과크기로 나타났다(effect size, ES=0.82, p<.001). 반면, 의사소통 명확성의 경우 2편의 연구가 포함되었고 큰 효과크기로 나타났지만 통계적으로 유의하지 않았다(ES=1.20, p<.066). 선행연구를 살펴보면 Kim과 Yoon [61]의 연구에서 표준화 환자를 활용한 시뮬레이션 교육이 국내 간호대학생 및 간호사의 의사소통능력에 큰 효과를 미치는 것으로 나타나(ES=1.07, 95% CI=0.62∼1.51) 본 연구 결과와 유사하였다. 그러나 Kang과 Jung [62]의 연구에서는, 국내 간호사를 대상으로 한 시뮬레이션 교육, 인수인계 교육, 자기주장훈련 등을 포함한 다양한 의사소통 교육에서 의사소통 명확성은 큰 효과크기(ES=1.00, 95% CI=0.66∼1.34), 의사소통능력은 중간 효과크기로 나타나(ES=0.68, 95% CI=0.58∼0.78), 본 연구와는 다른 결과로 나타났다. 이는, 본 연구가 시뮬레이션 교육 중재만 확인한 반면 Kang과 Jung [62]의 연구에서는 다양한 의사소통 교육 중재를 포함하였기 때문인 것으로 생각된다. 또한, 본 연구에서 의사소통 명확성의 효과에 대하여 포함된 연구는 2편으로, 적은 수의 연구를 포함하고 있어 결과를 일반화시키는 데 주의가 필요할 것이다. 특히 시뮬레이션 교육을 통한 의사소통 명확성의 효과를 파악한 국내·외 연구는 아직까지 미비한 실정으로 향후 의사소통 교육 프로그램의 근거와 방향성을 제시하기 위해 의사소통의 하위 변인에 대한 구체적인 효과를 검증한 연구가 필요할 것이다.
본 연구에서 시뮬레이션 교육이 간호대학생과 간호사의 의사소통에 미치는 효과에 대한 이질성 검정결과 이질성이 큰 것으로 나타나(I2=89.9%), 메타 ANOVA를 이용하여 원인을 파악하고자 하였다. 우선, 시뮬레이션 교육 대상자에 대해 살펴보면 간호사보다 간호대학생이 더 많았으며 3학년을 대상으로 한 연구가 가장 많았다. 하지만 메타분석 결과 1학년 집단에서 2.91로 효과크기가 가장 큰 것으로 나타났으며, 다음으로 3학년 집단의 효과크기 0.83, 4학년 집단의 효과크기 0.56 순으로 나타났다. 이는 기존의 간호교육에서 3학년과 4학년을 위주로 시뮬레이션 교육이 진행되었으나[63], 최근 의사소통의 중요성이 대두됨에 따라 1학년의 교과과정에도 시뮬레이션 교육을 통한 의사소통 교육이 시도되고 있으며 그 효과가 크다는 것을 알 수 있다. 그러나 메타분석에 포함된 1학년 대상의 연구 1개로 효과크기가 과대추정 된 결과로 볼 수 있어 해석상 주의가 필요할 것이다. 그럼에도 불구하고 메타분석에 포함된 1∼2학년을 대상으로 한 연구 모두에서 시뮬레이션 교육 효과에 대해 의사소통과 관련된 결과변수를 보고하고 있어 의사소통 향상을 위해서는 장기적인 교육이 필요함을 제시하고 있다. 이를 통해 안전하고 질 높은 간호의 기초를 마련할 수 있도록 해야 할 것이다.
의사소통의 효과를 보고한 연구에서 시뮬레이션 교육 중재에 사용된 시나리오는 성인간호학과 아동간호학에 관련된 시나리오가 대부분이었으며 시나리오 개수가 7∼9개의 경우 효과크기가 1.98로 가장 큰 것으로 나타났다. 시뮬레이션 교육 시나리오 개수에 따른 효과를 분석한 연구가 없어 직접적인 비교는 어려우나, Kang과 Jung [62]의 연구에서 간호사를 대상으로 한 의사소통 관련 중재 연구에서 5∼8회기의 교육을 진행했을 때 효과가 가장 높은 것으로 나타났다(ES=1.65, 95% CI=1.39∼1.91). 특히 의사소통은 지속적인 교육과 학습을 통해 향상될 수 있기 때문에[64], 다양한 시나리오를 바탕으로 비교적 장기간의 교육을 통하여 향상시키는 것이 필요하다.
시뮬레이션 교육이 의사소통능력에 미치는 효과를 보고한 연구를 살펴보면, 의사소통능력 측정을 위해 다양한 측정도구가 사용되었다. 특히 ‘대인간 의사소통능력 모델’을 토대로 개발된 대학생 및 성인의 생애능력 중 의사소통능력을 측정하기 위한 GICC를 사용하여 평가한 연구가 4편으로 가장 많았다[35,49, 52,53]. GICC를 사용한 연구는 모두 국내 연구였으며, 측정도구에 따른 효과크기는 0.20으로 가장 낮은 것으로 나타났다. 이 도구는 자가보고 방식으로 자기노출, 역지사지, 사회적 긴장완화, 주장력, 집중력, 상호작용 관리, 표현력, 지지, 즉시성, 효율성 사회적 조절성, 조리성, 목표간파, 반응력 및 잡음 통제력에 대한 내용을 포함하고 있다[65]. 의사소통이란 사람의 의사나 감정의 소통에 대한 의미를 가지고 있지만[66], 간호학에서 사용하는 의사소통은 협력과 조정의 의사소통, 환자와의 치료적 의사소통을 포함하고 있다[67]. 따라서, 시뮬레이션 교육을 통한 의사소통능력의 효과는 대인관계에서 이루어지는 의사소통능력보다는 간호사 업무의 특성에 따른 의사소통능력에 대한 평가가 이루어져야 할 것이다. 이는 메타분석에 포함된 Ha와 Jung [35]의 연구에서도 측정 도구의 문제에 대해 제시하고 있으며, Yang과 Hwang [68]의 연구에서도 시뮬레이션 상황에서 의사소통능력을 측정하는 데에는 적합하지 않다고 보고하고 있어 의사소통능력에 대한 적절한 측정도구 선택 및 측정도구 개발의 필요성을 제시하고 있다. 또한 의사소통능력을 측정하기 위해 사용된 기타 측정도구 중 관찰평가의 방식에서 효과크기가 1.33으로 제일 높게 나타났다. 따라서 자가보고 방식의 한계점을 보완하기 위해 객관성을 확보할 수 있는 관찰평가가 수행되거나 자가보고와 관찰평가가 함께 진행되는 것이 필요할 것이다.
본 연구에서 시뮬레이션 교육이 간호대학생과 간호사의 임상판단능력에 미치는 효과크기는 1.84로 큰 효과크기로 나타났다. 이는, 선행연구에서 시뮬레이션 교육이 국내·외 간호대학생의 임상판단에 미치는 효과에 대해 메타분석한 Lee [20]의 연구에서 효과크기 1.72 (95% CI=-0.73∼2.71)로 나타났으며, 국내 간호대학생과 간호사를 대상으로 한 Kim과 Ham [21]의 연구에서 효과크기 1.49 (95% CI=0.77∼2.21)로 큰 효과크기를 나타낸 선행연구의 결과와 유사한 결과이다.
그러나 본 연구에서 시뮬레이션 교육이 간호대학생과 간호사의 임상판단능력에 미치는 효과에 대한 이질성 검정결과 이질성이 큰 것으로 나타나(I2=94.7%), 메타 ANOVA를 이용하여 원인을 파악하고자 하였다. 우선, 시뮬레이션 교육 대상자에 대해 살펴보면 임상판단능력에 대한 시뮬레이션 교육의 효과를 파악하기 위해 임상실습 경험이 있는 3학년 이상의 학생 교육이 진행되었으며, 4학년 집단에서 3.53으로 효과크기가 가장 큰 것으로 나타났다. 그러나 메타분석에 포함된 4학년 대상의 연구 1개로 효과크기가 과대추정된 결과로 볼 수 있어 해석상 주의가 필요할 것이다. 그럼에도 불구하고 간호사를 대상으로 한 연구보다 3∼4학년을 대상으로 한 연구에서 더 큰 효과크기를 나타내어 간호대학생을 대상으로 한 시뮬레이션 교육이 임상판단능력을 향상시키는 데 더욱 효과적임을 알 수 있다. 따라서, 시뮬레이션 교육이 임상 상황을 완전히 대체할 수는 없지만 학부교육과정을 통해 임상판단능력을 향상시킬 수 있도록 노력해야 할 것이다.
임상판단능력의 효과를 보고한 연구에서 시뮬레이션 교육 중재에 사용된 시나리오는 개수에 대해 살펴보면, 운영된 시나리오 개수가 4∼6개의 경우 효과크기가 2.77로 가장 큰 것으로 나타났다. 이는, 임상판단능력도 의사소통과 마찬가지로 다양한 시나리오를 통한 교육의 중요성을 시사하고 있다. 따라서, 추후 임상판단능력을 향상시키기 위한 시뮬레이션 교육 프로그램 개발 시 이를 고려하여야 할 것이다.
임상판단능력에 대한 측정도구를 살펴보면, 메타분석에 포함된 7편의 연구 중 5편에서 임상판단능력을 측정하기 위해 LCJR을 사용하였으며 큰 효과크기로 나타났다(ES=2.39). 이와 비교하여 Ha와 Koh [57]의 연구에서는 연구자가 개발한 도구로 사용하였으며 효과크기 0.81로 나타나 LCJR을 사용한 연구와 비교할 때 낮은 효과크기를 나타내고 있어 측정도구의 중요성에 대해 알 수 있다. 따라서 시뮬레이션 교육에서 통해 측정하고자 하는 것의 개념을 명확히 하여, 변수를 측정하기 위한 적절한 측정도구를 선택하고 필요시 일관성 있는 측정 도구의 개발이 요구될 것으로 생각된다.
이와 같이 본 연구에서 시뮬레이션 교육이 간호대학생과 간호사의 의사소통과 임상판단능력에 미치는 효과에 대해 파악하고, 높은 이질성의 원인을 파악하기 위해 연구 설계 측면에 대한 하위 분석을 시행하였다. 본 연구의 체계적 문헌고찰에 포함된 연구에서 시뮬레이션 교육은 운영에 있어 중재기간, 시나리오 개수, 운영시간의 많은 편차를 보이고, 프리브리핑과 디브리핑 운영에도 연구에 따라 많은 차이를 보이고 있었다. 일부 연구에서는 시뮬레이션 중재관련 내용, 프리브리핑 및 디브리핑의 구성과 운영 내용에 대해 정확한 기술을 하지 않았다. 따라서, 시뮬레이션 교육에 대한 효과를 보고하는 연구에서는 향후 중재 프로그램 개발의 객관적인 근거로 사용될 수 있으므로 연구 결과를 누락하지 않도록 해야 할 것이다.
본 연구는 시뮬레이션 교육이 간호대학생과 간호사의 의사소통과 임상판단능력 향상에 효과가 있다는 근거를 마련하였다. 그러나, 측정결과 값의 범위가 크고 결측값이 많은 것과 관련하여 출판편향이 있을 수 있다는 점에서 해석상 주의가 필요할 것이다. 또한, 각 문헌의 이질성이 높은 것으로 나타났는데, 이는 시뮬레이션 교육의 다양한 중재시간, 횟수, 사용한 도구 등이 다르기 때문이므로, 시뮬레이션 교육 효과에 대한 질적 향상을 위해 표준화된 도구의 개발이나 반복연구가 필요할 것이다. 또한 시뮬레이션 교육 프로그램에 대한 중재와 결과 간의 명확한 관련성을 설명하고 가장 높은 수준의 근거를 제공하기 위해서는[69], 무작위대조군 실험연구를 통한 효과평가 연구가 요구될 것이다.
결론 및 제언
본 연구는 시뮬레이션 교육이 간호대학생과 간호사의 의사소통과 임상판단에 미치는 효과를 확인하기 위하여 체계적 문헌고찰 및 메타분석을 시행하였다. 시뮬레이션 교육은 의사소통 향상에 중간 수준의 효과크기가 있었으며, 임상판단능력 향상에는 큰 크기의 효과가 있는 것으로 나타나 시뮬레이션 교육은 의사소통과 임상판단능력 향상에 유용한 방법임을 알 수 있다. 또한, 시뮬레이션 교육에 사용된 시나리오, 교육 대상자 및 측정도구에 따른 효과크기를 분석하여 시뮬레이션 교육 프로그램 개발의 기초자료를 마련한 것에 연구의 의의가 있다. 본 연구 결과를 바탕으로 간호대학생과 간호사의 의사소통능력 및 임상판단능력을 향상시키기 위한 시뮬레이션 교육은 일회성이 아닌 단계적이고 장기적인 교육 프로그램을 개발하여 적용할 것을 제언한다. 교육 프로그램은 다양한 시나리오를 바탕으로 하여 점진적으로 의사소통능력 및 임상판단능력을 향상시킬 수 있도록 구성할 필요가 있으며, 특히 간호학과에서는 1학년 과정에서부터 연속성과 체계성을 가지고 의사소통능력 및 임상판단능력을 개발할 수 있도록 간호교육의 커리큘럼을 구성할 필요가 있을 것이다. 또한, 의사소통능력 평가는 자가보고와 관찰평가를 동시에 실시하여 적절한 피드백을 제공할 필요가 있으므로, 의사소통능력에 대한 정형화된 평가도구를 개발하여 보다 객관적인 중재 효과를 검증할 것을 제언한다.




