간호대학생을 위한 전문직 간 교육 프로그램에 대한 체계적 문헌고찰
Interprofessional Education Programs for Nursing Students: A Systematic Review
Article information
Trans Abstract
Purpose
The purpose of this study was to investigate how interprofessional education has been designed, implemented, and evaluated in undergraduate programs in nursing through a systematic review.
Methods
The literature was searched using the PubMed, CINAHL, EMBASE, and Cochrane central databases to identify interventional studies including teaching-learning activities among nursing students and other disciplines in English between January 2000 and May 2017. Thirty studies were selected for the analysis.
Results
Twenty-four studies out of 30 were designed as a pre-post, no control group, quasi-experimental study design. Interprofessional education learners were primarily engaged in medicine, physical therapy, dentistry, occupational therapy, pharmacy, and respiratory therapy. Patient care related activity was the most frequently selected topic and simulation was the most common teaching-learning method. Evaluation of learning outcomes was mainly based on the aspects of teams and collaboration, professional identity, roles and responsibilities, patient care, and communication skills. Nursing students in 26 out of the 30 reviewed studies were found to benefit from interprofessional education, with outcome effects primarily related to changes in learning outcomes.
Conclusion
The development and integration of interprofessional education with collaborative practices may offer opportunities in nursing education for training professional nurses of the future.
서 론
연구의 필요성
전문직 간 교육(interprofessional education)은 “둘 혹은 그 이상의 전문가들이 함께 배우고, 상대방으로부터 배우고, 그리고 서로에 대하여 배우는 과정”을 의미한다(Centre for the Advancement of Interprofessional Education, 2002). 그러므로 다른 교육 배경을 가진 둘 이상의 보건의료 전문가들 사이의 장벽과 갈등을 제거하고, 모든 직업에 대한 올바른 가치와 태도를 함양시키므로 양질의 환자중심 돌봄(patient centered care)을 촉진시킨다는 장점이 있다(World Health Organization, 1988). 또한 전문직 간 교육이 임상에서 실제 서로의 역할을 잘 이해하며, 팀워크, 의사소통 및 협업역량을 극대화 시킨다는 연구 결과들이 지속적으로 보고됨에 따라(D’amour & Oandasan, 2005), 유럽을 비롯한 캐나다, 호주, 미국 등의 국가에서는 면허취득 전 단계부터 정부와 각 학교 차원에서 전문직 간 교육을 실시하기 위해 많은 노력을 기울이고 있다(Hammick, Freeth, Koppel, Reeves, & Barr, 2007). 캐나다의 경우에는 2001년 University of British Columbia에 보건훈련대학을 설치하여 보건의료전공 학생들에게 전문직 간 교육을 처음으로 실시하였으며, 미국 또한 2009년에 치과대학, 의과대학, 간호대학, 약학대학 등의 여러 보건의료 관련 대학들이 Interprofessional Education Collaboration (IPEC)라는 조직을 설립하여 전문직이 갖추어야 할 핵심역량을 제시하고, 역량 개발을 위한 다양한 교육적 시도를 지속해왔다.
최근 간호교육에서도 환자간호에 대한 효율적인 접근과 환자중심 돌봄이라는 공동목표를 실현하기 위해 다른 전문가들과 협업이 필수적이며, 이를 위한 간호교육의 혁신적인 변화를 요구하고 있다(Captuti, 2016). 특히 간호사는 모든 보건의료 전문가 및 환자와의 관계에 있어 매개체 역할을 하므로 원활하고 정확한 의사소통을 위한 협업역량이 매우 중요하다고 할 수 있다(Kim et al., 2012). 국내에서도 최근 간호교육에서 전문직 간 교육의 중요성 및 이에 대한 현황과 발전방향(Han, 2017; Kim, Hwang, & Shin, 2017)에 관한 연구들이 발표되고 있다. 그러나 실제 교육현장에서 전문직 간 교육을 도입한 사례나 효과에 대한 선행연구는 전무한 실정이며, 임상에 있는 의사 86%와 간호사 62%가 전문직 간 교육에 대한 경험이 전혀 없는 것으로 보고되고 있다(Lee, Ahn, Moon, & Han, 2014). 이는 전문직 간 교육을 통해 보건의료전공 학생들의 전문직 정체성 및 협업역량을 개발시키고, 환자중심의 보건의료 서비스를 제공하기 위해 많은 노력을 기울이고 있는 국외와 달리(Barr, Bull, & Rooney, 2015), 국내에서는 아직 이에 대한 적극적인 논의 및 도입이 이루어지지 않고 있는 실정이다.
이제는 간호교육에서도 임상에서 강조되는 전문직 정체성 및 팀워크와 협업, 의사소통 능력을 개발하기 위해 많은 노력을 기울여야 할 시점이다. 따라서 본 연구에서는 간호대학생이 포함된 전문직 간 교육프로그램의 전반적인 특성을 분석하여, 향후 체계화된 교육프로그램을 설계하고 개발하기 위한 기초자료를 제시하고자 한다.
연구 방법
연구 설계
본 연구는 간호대학생이 포함된 전문직 간 교육활동 및 교육프로그램을 분석하기 위한 체계적 문헌고찰 연구이다. 본 연구의 설계방식은 한국보건의료연구원의 체계적 문헌고찰 매뉴얼(Kim et al., 2011)의 연구방법에 따라 진행하였다.
핵심 질문
핵심질문은 Participants, Intervention, Comparison, Outcome (PICO)의 기준을 이용하여 구체화하였으며 다음과 같다.
∙ 연구대상(Participants): 간호대학생
∙ 중재(Interventions): 전문직 간 교육과정 및 프로그램화된 교육활동
∙ 결과(Outcomes): 전문직 간 교육의 목표이자 도구를 사용하여 측정가능한 팀워크와 협력, 전문직 정체성, 역할과 책무성, 환자중심성, 의사소통 기술 등과 같은 종속변수
문헌 검색 전략
문헌 검색과 분석은 국외에서 전문직 간 교육에 대한 연구가 활발하게 이루어지기 시작한 시점인 2000년 1월 1일부터 2017년 5월 31일까지 실시하였다(Green, 2014). 데이터베이스는 미국국립의학도서관(National Library of Medicine, NLM)이 제시한 COSI (Core, Standard, Ideal)모델을 근거로 Core DB에 해당하는 PubMed, EMBASE, Cochrane Central과 Standard DB 가운데 CINAHL을 통해 검색하였다. 문헌 검색 시 핵심어(주제어)는 ‘interprofessional education’, ‘interprofessional program’, ‘interprofessional practice’, ‘interprofessional curriculum’, ‘interprofessional course’, ‘nursing students’ 로 사용하였다.
검색된 문헌 중 전문직 간 교육과정 및 프로그램화된 교육활동에 간호대학생이 포함된 중재 연구와 전문직 간 교육 프로그램에 대한 특성(주제, 대상자, 교육내용, 교육방법, 평가도구)을 파악할 수 있으며 객관적인 평가를 시행한 연구 가운데 전문을 확보할 수 있는 문헌을 선정하였다. 배제 기준은 회색문헌, 영어로 출판되지 않은 문헌, 연구대상자에 간호대학생이 포함되지 않은 연구, 질적연구(사례연구, 면담에 의한 서술연구)를 시행한 문헌은 배제하였다. 그러나 혼합연구 방법을 사용한 문헌일 경우 전문을 검토하여 양적연구의 비중이 크고 교육프로그램에 대한 특성 및 효과를 명확하게 파악할 수 있는 문헌들은 연구자간의 충분한 논의를 거쳐 포함시켰다.
분석문헌 선택과정
단계별 문헌선택과정의 현황을 자세히 기술하기 위하여 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)의 흐름도를 사용하였다(Moher, Liberati, Tetzlaff, Altman, 2009). 국외 데이터베이스를 통해서 검색된 문헌들은 총 1670편이 검색되었다. 중복 검사를 시행하여 1,206편을 제외한 총 464편의 문헌이 채택되었고 제목과 초록을 검토하여 연구주제, 대상과 관련성이 있는 143편의 논문에 대하여 문헌선정 및 제외기준을 적용하였다. 이 중 중재연구가 아닌 문헌 67편, 전문직 간 교육프로그램의 특성을 파악할 수 없는 문헌 45편, 전문이 공개되지 않는 문헌 1편으로 총 113편이 제외되어 최종 30편의 국외 문헌이 선정되었다(Figure 1). 모든 문헌선정과 배제과정은 연구자 2인에 의해 독립적으로 시행되었다.
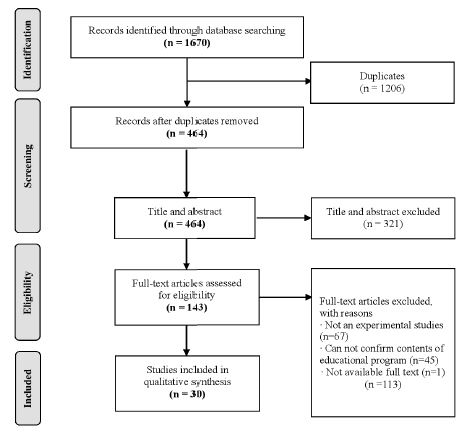
PRISMA flow chart of study selection.
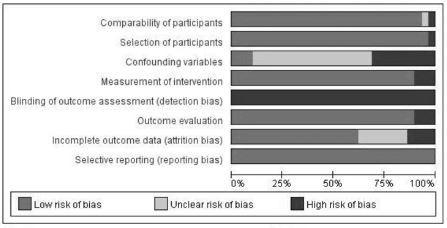
Risk of bias graph: Review authors’ judgments about each risk of bias item presented as percentages across all included studies.
자료의 질 평가
본 연구에서 최종 선정된 문헌의 질 평가는 Risk of Bias (Cochrane RoB)와 Risk of Bias Assessment tool for Non-randomized Study (RoBANS)를 활용하여 시행하였다(Kim, 2013). 1편의 논문은 무작위대조연구로 RoB로 평가하였으며, 나머지 29편의 논문은 비무작위 연구의 비뚤림 위험 평가를 위한 도구인 RoBANS로 ‘대상군 비교가능성’, ‘대상군 선정’, ‘교란변수’, ‘노출측정’, ‘평가자의 눈가림’, ‘결과평가’, ‘불완전한 결과자료’, ‘선택적 결과보고’의 8가지 항목에 대한 비뚤림 위험을 평가하였다. 2인의 연구자가 독립적으로 8가지 항목에 대하여 ‘낮음’, ‘높음’, ‘불확실’로 평가하였고, 불일치되는 부분은 논의를 통해 최종적으로 결과를 도출하였다.
연구 결과
문헌의 일반적 특성
총 30편의 연구논문 중 20편(66.7%)은 2010년 이후에 발표되었다. 국가별 논문 수는 미국이 9편(30.0%), 캐나다가 7편(22.6%)으로 가장 많았고, 그 다음으로는 스웨덴과 영국에서 각각 4편(13.3%)의 논문이 발표되었다. 그 외 싱가포르, 홍콩, 벨기에, 한국, 중국, 호주에서 각각 1편씩 발표되었다.
간호대학생과 함께 전문직 간 교육프로그램에 참여한 학습자는 의과대학생이 26편(86.7%)으로 가장 많았고, 물리치료 전공학생이 9편(30.0%), 작업치료 전공학생이 6편(20.0%), 치과대학생이 6편(20.0%), 약학대학생이 5편(16.7%), 호흡치료 전공학생이 2편(6.7%) 이었다. 그 외 신학대학생, 사회복지 전공학생, 조산학 전공학생, 식품영양학 전공학생, 방사선학 전공학생 등이 포함되었다.
연구 설계는 대조군이 없는 단일군 전후 유사실험연구가 18편(60.0%)으로 가장 많았고, 혼합연구 9편(30.0%), 대조군이 있는 유사실험연구 2편(6.7%), 무작위대조연구가 1편(3.3%)이었다.
교육운영 장소로는 학교에서 전문직 간 교육을 실시한 경우가 20편(66.7%), 병원에서 실시한 경우가 7편(23.3%)으로 가장 많았고, 그 외 학교·병원에서 공동으로 운영한 경우가 1편(3.3%), 보건관련 센터와 박물관에서 교육을 운영한 경우가 각각 1편씩(3.3%) 발표되었다(Table 1).

Characteristics of Interprofessional Education Program Systematic Review Articles
(N=30)
대상 논문의 질 평가 결과
RoB도구를 사용하여 평가한 1편의 문헌은 7개의 영역 중 ‘무작위 배정순서 생성’, ‘불충분한 결과자료’, ‘선택적 보고’, ‘그 외 비뚤임’ 영역에서 비뚤임의 위험이 낮았다. 그 외 ‘연구 참여자, 연구자에 대한 눈가림’, ‘결과평가에 대한 눈가림’ 영역에서는 연구 참여자와 평가자의 눈가림이 이루어지지 않았고, 자가보고식의 결과 평가로 인해서 비뚤임의 위험이 높았으며 ‘배정순서 은폐’ 영역에 대해서는 언급되지 않았다.
나머지 29편의 문헌은 RoBANS 도구를 사용하여 평가하였다. ‘대상군 비교가능성’ 영역에서 25편의 문헌은 단일군 전후 비교연구로 중재에 대한 노출 전후의 대상자가 동일하였고, 4편의 비동등성 대조군 사전사후 검사 설계 문헌에서는 2편의 문헌이 대조군과 실험군간의 동질성을 검증하여 비뚤림 위험이 낮았으며 2편의 문헌은 대조군과 실험군 간의 동질성을 검증을 시행하지 않았다. ‘대상군 선정’ 영역에서는 28편의 연구에서 자료를 전향적으로 모집하였고 포함기준에 해당되는 대상자를 임의로 선택하거나 누락시키지 않았다. 그러나 1편의 논문에서는 대상자의 일부가 후향적으로 선정되어 비뚤임의 위험이 높았다. ‘교란변수’ 영역에서는 오직 3편의 문헌만이 교란변수를 통제하기 위해 디자인 단계에서 동질성 검증을 시행하여 대조군을 선정하거나 분석단계에서 공변량 분석을 실시하였다. ‘노출측정’ 영역에서는 3편의 문헌이 프로그램의 효과를 평가하기 위해 객관성이 입증되지 않은 자체 개발된 도구를 사용하여 비뚤임의 위험이 높게 평가되었다. ‘평가자의 눈가림’ 영역에서는 모든 연구에서 자가보고설문을 통해 중재의 효과를 평가하였으므로 비뚤임의 위험이 높다고 볼 수 있다. ‘결과평가’ 영역은 26편의 문헌이 신뢰도와 타당도가 입증된 도구를 사용하였고, 3편의 문헌에서 도구의 신뢰도와 타당도를 언급하지 않았다. ‘불완전한 결과자료’ 영역에서는 두 군의 탈락자 수의 차이가 큰 문헌이 4편이었고, 탈락자의 수가 명확하게 제시되지 않은 문헌이 7편이었다. ‘선택적 결과 보고’ 영역은 모든 문헌에서 예상되는 주요 결과가 모두 포함되어 있어 비뚤임의 위험이 적은 것으로 판정하였다.
전문직 간 교육프로그램의 특성
전문직 간 교육의 주제는 환자돌봄과 관련된 주제가 22편(73.3%)으로 가장 많았다. 그 다음으로는 팀워크 관련 주제가 15편(16.7%), 환자안전 관련 주제가 4편(13.3%)이었으며, 그 외 통증관리, 재난관리, 미술작품 묘사 등이 있었다. 환자돌봄과 관련된 소주제로는 신경계 환자관리(예: seizure, parkinson’s patient, stroke patient, confused elderly patients), 심혈관계 환자관리(예: atrial fibrillation, cardiac resuscitation skills, chest pain, emergency cardiac event), 호흡기계 환자관리(예: severe acute respiratory syndrome, tension pneumothorax, asthma, chronic obstructive pulmonary disease), 영유아 환자관리(예: febrile illness, viral upper respiratory tract infection, chronic asthma), 소화기계 환자관리(예: intra-abdominal hemorrhage, appendectomy, splenectomy), 수술 전후 환자관리(예: acute & elective orthopaedic conditions, peri-operative care), 감염 환자관리(예: sepsis, wound infection), 말기암 환자관리(예: oncology palliative care), 과민반응 환자관리(예: anaphylaxis, anesthetic toxicity, overdose insulin), 일상생활 관리(예: mobility, nutrition, feeding, self care)와 같이 임상에서 보편적으로 접할 수 있는 다양한 주제가 활용되었다. 팀워크 관련 소주제로는 의사소통 기술 향상, 전문직 간 원만한 관계 형성에 관한 주제가 있었고, 환자안전 관련 소주제로는 인적오류, 의료오류, 환자안전 개선방법에 관한 주제가 있었다.
교육 운영기간은 반나절부터 2년까지 매우 다양했으며 1∼3일 과정 10편, 1∼2주 과정 8편, 1∼2개월 과정 1편, 1∼3년 과정이 10편이었다. 그 외 1편의 연구에서 9개월 과정이 있었다.
교육방법은 시뮬레이션이 14편(46.7%)으로 가장 많이 활용되었다. 이외에도 임상활동 8편(26.7%), 사례연구 5편(16.7%), 토론 4편(3.3%), 문제바탕학습 2편(6.7%) 순으로 나타났으며, 가상학습, 팀 바탕학습, 역할극 등 다양한 교육방법이 활용되고 있었다(Table 1).
전문직 간 교육프로그램 평가의 특성
최종 선정된 연구논문에서 모든 전문직 간 교육은 팀 형태의 수업방식으로 진행되었으나, 평가는 자가보고식의 개인평가로 이루어졌다. 학습성과에 대한 평가항목으로는 팀워크와 협력을 평가한 연구가 22편(77.3%)이었으며, 전문직 정체성 17편(56.7%), 역할과 책무성 13편(43.3%), 환자중심성 10편(33.3%), 의사소통 기술 9편(30.0%), 임상지식을 평가한 연구가 7편(23.3%)이었다. 그 외 팀 활동 경험에 대한 만족도, 전문직 간 교육에 대한 태도, 리더십 등이 있었다. 이러한 평가항목을 측정하기 위해 사용한 도구는 문헌마다 매우 다양하였으며, 주로 The Readiness for Inter-professional Learning Scale (RIPLS)을 사용한 연구가 8편(26.7%), Interdisciplinary Education Perceptions Scale (IEPS)을 사용한 연구가 2편(6.7%)이었다. 그 외의 연구에서는 연구자들이 자체 개발한 설문을 사용한 것으로 나타났다(Table 2).

Reported Outcomes of Interprofessional Education Program Interventions
(N=30)
논 의
본 연구는 간호대학생이 포함된 전문직 간 교육프로그램의 특성을 체계적으로 분석하고, 향후 간호교육에 적용할 수 있는 전문직 간 교육프로그램을 설계하고 개발하기 위한 기초자료를 제공하고자 시행되었다.
전문직 간 교육은 미국, 캐나다, 스웨덴, 독일과 같이 현재 전문직 간 교육을 적극적으로 시행하고 있는 나라에서 연구가 활발하게 이루어지고 있으며, 2000년 이후부터 전문직 간 교육에 대한 논문수가 점차적으로 증가하고 있는 추세이다(Green, 2014). 국내에서도 역시 전문직 간 교육의 필요성이 대두되고 있으며(Han, 2017; Yoon & Lee, 2010), 실제 간호대학 교수자들 역시 전문직 간 교육을 시행할 의향이 높은 것으로 나타났다(Kim et al., 2017). 그러나 국내에서 전문직 간 교육을 시도하고 그 효과를 검정한 연구는 단 1편에 불과하였다(Hwang et al., 2016). 이 연구에서는 마지막 학기의 간호대학생, 의과대학생, 한의과대학생 233명을 대상으로 환자안전 역량을 향상시키기 위해 하루과정으로 5시간 30분 동안 강의식 수업과 실습을 병행하여 운영하였다. 비록 짧은 교육시간 이었지만 보건의료전공 학생들의 환자안전 역량을 효과적으로 향상시켰으며, 교육 2개월 후 8명의 간호대학생들에게 시행한 인터뷰 결과에서도 안전문제에 대해 서로 정보를 교환하고 관심을 집중시키는데 긍정적인 결과를 가져왔다고 보고하고 있다. 이는 4∼6시간의 짧은 전문직 간 교육 과정으로도 교육대상자들의 팀워크와 의사소통 능력을 효과적으로 향상시켰다고 보고한 국외논문의 결과와도 일치하는 바이다(Klugman, Peel, & Backmann-Mendez, 2011; Luctkae et al., 2010; Paige et al., 2014).
연구설계 방법은 30편의 문헌 중 25편이 단일군 전후 유사실험연구였다. 그 이유는 학생들에게 실험군과 대조군을 스스로 선택하게 하였으나 학생들 모두가 전문직 간 교육 프로그램에 참여하기를 원하는 경우가 많았고(Klugman et al., 2011), 동일한 실험군과 대조군을 모집하는데 어려움이 있었으며(Hallin, Kiessling, Waldner, & Henriksson, 2009; Paige et al., 2014), 다양한 분야의 전공학생들이 함께 교육을 받아야 했으므로 시간적, 제도적인 제약의 문제가 있었기 때문에(Paige et al., 2014) 무작위대조군 실험연구를 설계하는데 어려움이 있었다고 설명하고 있다. 그러나 교육프로그램에 대한 중재와 결과간의 명확한 관련성을 설명하고 가장 높은 수준의 근거를 제공하기 위해서는(Bench, Day, & Metcalfe, 2013), 향후 많은 연구자들이 전문직 간 교육에 대한 무작위대조군 실험연구에 도전할 필요가 있다고 사료된다.
본 연구에서 선정된 문헌의 질 평가 결과에서는 30편의 문헌 모두 자기보고식의 평가를 시행함으로써 평가자의 눈가림이 이루어지지 않았고, 주요 교란변수를 확인하지 않거나 불확실한 문헌이 26편이나 되었다. 그러므로 추후 전문직 간 교육 프로그램 운영시 이런 질 평가 부분들을 충분히 고려하여 교육프로그램의 질 향상을 위한 노력을 기울여야 할 것이다.
간호대학생과 함께 전문직 간 교육에 참여한 학습자는 의과대학생이 가장 많았다. 이들은 실제 임상에서 환자와 면밀하게 상호작용하며 환자치료에 가장 많은 시간을 할애하고 있는 집단으로, 의사와 간호사의 협업정도가 환자의 만족도 및 치료결과에 직결되기 때문이다(Vazirani, Hays, Shapiro, & Cowan, 2005). 실제 국외에서 시행된 체계적 문헌고찰 연구에서도 전문직 간 교육 프로그램은 의사와 간호사의 팀워크 및 협업역량을 향상시키고, 만성질환자들의 생존률을 높일 뿐 아니라 환자들의 신체적·정신적·사회적 기능을 향상시키는데 직접적인 영향을 주었다고 보고하고 있다(Martin, Ummenhofer, Manser, & Spirig, 2010). 교육주제 역시 주로 병원에서 쉽게 접할 수 있는 응급환자나 급성기 환자의 실제사례를 제시하고, 환자돌봄을 제공하는 경우가 많았다. 그러나 현재 우리사회는 초고령화 사회에 진입하고 있어 이로 인한 만성질환자수가 급격하게 증가하고 있다. 그러므로 Phillips, Hall과 Irving (2016)은 전문직 간 교육은 병원 뿐 만 아니라 지역사회 기반으로도 확대되어야 함을 강조하고 있다. 따라서 전문직 간 교육 역시 병원 셋팅에서 뿐 아니라 건강증진 및 예방을 목적으로 하는 지역사회 기반의 교육프로그램으로 다양하게 개발해야 할 것이다.
전문직 간 교육방법은 학생들이 스스로 문제 해결에 필요한 정보를 탐색하고 활용하여 의사소통, 팀워크 등의 역량을 효과적으로 습득할 수 있는 시뮬레이션, 임상활동, 사례연구, 토론, 문제바탕학습 등 협동학습에 기반한 수업형태가 많았다(Interprofessional education collaborative expert panel, 2011). 교육의 학습성과로는 교육 참여자들의 팀워크와 협력, 전문직 정체성, 역할과 책무성, 환자중심성, 의사소통 기술을 주로 평가하였다. 이중 팀워크와 협력 부분의 점수가 가장 많이 향상되었는데, 이는 교육을 통해 실제 학습자들에게 협업을 경험할 수 있는 기회를 제공함으로써 직군간의 이해도를 높이고 좋은 협력관계를 형성하는 것이 전문직 간 교육의 궁극적인 목적이기 때문일 것이다(Kim et al., 2017).
마지막으로, 전문직 간 교육의 효과는 30편의 논문 중 26편에서 모든 학습성과가 유의하게 향상되었으나, 나머지 4편의 연구에서는 ‘자아정체성’, ‘다른 직군에 대한 이해도’, ‘환자안전 관련 지식’ 등 유의하지 않은 일부 항목들이 있었다. 자아정체성 항목은 의과대학생들에게 유의하지 않았는데, 이들은 전문직 간 교육 시행 전부터 다른 직군에 비해 전문직 정체성 점수가 높았기 때문에 교육 후 점수가 유의하게 향상되지 않은 것으로 판단된다(McGettigan & McKendree, 2015). 다른 직군에 대한 이해도 항목은 평가 특성상 개인의 주관성이 결과에 많은 영향을 주는 부분이었으나 이를 객관화된 도구로 측정한 것은 무리가 있었다고 사료되며(Mohaupt et al., 2012), 환자안전 관련 지식 항목은 보건의료 종사자들에게 강조되는 부분으로 이미 전문직 간 교육 시행 전부터 지식 및 기술수준이 높아 교육 후 점수가 유의하게 향상되지 않았다고 판단된다(Nagelkerk et al., 2014; Whelan, Spencer, & Rooney, 2008).
결론 및 제언
본 연구에서는 체계적 문헌고찰을 통해 전문직 간 교육이 간호대학생을 비롯한 보건의료전공 학생들의 전문직 정체성, 팀워크와 협력, 의사소통 기술을 효과적으로 향상시키며, 더 나아가 환자중심의 보건의료 서비스를 가능하게 해주는 원동력임을 확인할 수 있었다. 그럼에도 불구하고 전문직 간 교육은 구조적 요인(예; 학사일정의 어려움), 태도문제(예; 변화하지 않으려는 태도), 교육과정/교수법(예; 여러 가지 역할을 담당하는 교수훈련, 새로운 형태의 교수와 학습의 요구), 전문직업성/학제(예; 타 전문직종에 대한 지식과 이해부족, 전문직 간 다른 언어와 개념)와 같은 장애요인들로 인하여 실제 교육이 실행되기까지 많은 어려움이 있었다(Parsell & Bligh, 1999). 그러므로 국내에서도 전문직 간 교육의 활성화를 위해서는 교육의 중요성 및 필요성에 대한 인식이 향상되어야 하며, 교육과정 도입과 개발에 대한 높은 장벽을 낮추는 노력이 무엇보다도 우선시 되어야 할 것이다.
본 연구는 전문직 간 교육프로그램의 전반적인 특성을 확인하는데 초점을 두고 문헌고찰을 시행하였으므로 무작위대조군 실험연구 뿐 아니라 유사실험연구 역시 포함되었으므로 교육의 효과를 해석하는데 주의를 기울일 필요가 있다. 그러나 간호대학생을 포함한 전문직 간 프로그램의 특성을 체계적으로 고찰하고, 추후 교육프로그램을 개발하기 위한 근거자료를 마련하기 위해 국내에서 처음으로 전문직 간 교육프로그램에 대한 체계적 문헌고찰이 시도되었다는 점에서 의의를 찾을 수 있을 것이다.
본 연구 결과를 바탕으로 간호대학생들의 전문직 정체성과, 팀워크, 의사소통 및 협업역량을 향상시키기 위한 다양한 주제의 전문직 간 교육프로그램을 개발하고, 실제 적용하여 교육의 효과를 검정하는 후속 연구를 제언한다.
References
Barr, J., Bull, R., & Rooney, K. (2015). Developing a patient focussed professional identity: An exploratory investigation of medical students’ encounters with patient partnership in learning. Advances in Health Sciences Education, 20(2), 325-338.
Barr J., Bull R., et al, Rooney K.. 2015;Developing a patient focussed professional identity: An exploratory investigation of medical students’ encounters with patient partnership in learning. Advances in Health Sciences Education 20(2):325–338. 10.1007/s10459-014-9530-8.Bench, S., Day, T., & Metcalfe, A. (2013). Randomised controlled trials: An introduction for nurse researchers. Nurse Researcher, 20(5), 38-44.
Bench S., Day T., et al, Metcalfe A.. 2013;Randomised controlled trials: An introduction for nurse researchers. Nurse Researcher 20(5):38–44. 10.7748/nr2013.05.20.5.38.e312.Caputi L. (2016). Innovations in nursing education: Building the future of nursing (1st ed). United States: National League for Nursing.
Caputi L.. 2016. Innovations in nursing education: Building the future of nursing (1st ed) United States: National League for Nursing.Centre for the advancement in interprofessional education. (2002). Interprofessional education - A definition. Retreived from http://www.caipe.org.
Centre for the advancement in interprofessional education. 2002. Interprofessional education - A definition Retreived from http://www.caipe.org.D'amour, D., & Oandasan, I. (2005). Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. Journal of Interprofessional Care, 19(1), 8-20.
D'amour D., et al, Oandasan I.. 2005;Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. Journal of Interprofessional Care 19(1):8–20. 10.1080/13561820500081604.Green, C. (2014). The making of the interprofessional arena in the United Kingdom: A social and political history. Journal of Interprofessional Care, 28(2), 116-122.
Green C.. 2014;The making of the interprofessional arena in the United Kingdom: A social and political history. Journal of Interprofessional Care 28(2):116–122. 10.3109/13561820.2013.867840.Hallin, K., Kiessling, A., Waldner, A., & Henriksson, P. (2009). Active interprofessional education in a patient based setting increases perceived collaborative and professional competence. International Journal of Education in the Health Science, 31(2), 151-157.
Hallin K., Kiessling A., Waldner A., et al, Henriksson P.. 2009;Active interprofessional education in a patient based setting increases perceived collaborative and professional competence. International Journal of Education in the Health Science 31(2):151–157. 10.1080/01421590802216258.Hammick, M., Freeth, D., Koppel, I., Reeves, S., & Barr, H. (2007). A best evidence systematic review of interprofessional education: BEME Guide no. 9. International Journal of Education in the Health Science, 29(8), 735-751.
Hammick M., Freeth D., Koppel I., Reeves S., et al, Barr H.. 2007;A best evidence systematic review of interprofessional education: BEME Guide no. 9. International Journal of Education in the Health Science 29(8):735–751. 10.1080/01421590701682576.Han, H. Y. (2017). Interprofessional education in medical education: Can we break the silos?. Korean Medical Education Review, 19(1), 1-9.
Han H. Y.. 2017;Interprofessional education in medical education: Can we break the silos? Korean Medical Education Review 19(1):1–9. 10.17496/kmer.2017.19.1.1.Hwang, J. I., Yoon, T. Y., Jin, H. J., Park, Y., Park, J. Y., & Lee, B. J. (2016). Patient safety competence for final-year health professional students: Perceptions of effectiveness of an interprofessional education course. Journal of Interprofessional Care, 30(6), 732-738.
Hwang J. I., Yoon T. Y., Jin H. J., Park Y., Park J. Y., et al, Lee B. J.. 2016;Patient safety competence for final-year health professional students: Perceptions of effectiveness of an interprofessional education course. Journal of Interprofessional Care 30(6):732–738. 10.1080/13561820.2016.1218446.Kim, K. H., Hwang, E. H., & Shin, S. J. (2017). Current status and future direction of interprofessional education in nursing education. Korean Medical Education Review, 19(1), 18-24.
Kim K. H., Hwang E. H., et al, Shin S. J.. 2017;Current status and future direction of interprofessional education in nursing education. Korean Medical Education Review 19(1):18–24. 10.17496/kmer.2017.19.1.18.Kim, K. J., Han, J. S., Seo, M. S., Jang, B. H., Park, M. M., Ham, H. M., et al. (2012). Relationship between intra-organizational communication satisfaction and safety attitude of nurses. Journal of Korean Academy of Nursing Administration, 18(2), 213-221.
Kim K. J., Han J. S., Seo M. S., Jang B. H., Park M. M., Ham H. M., et al. 2012;Relationship between intra-organizational communication satisfaction and safety attitude of nurses. Journal of Korean Academy of Nursing Administration 18(2):213–221. 10.11111/jkana.2012.18.2.213.Kim, S. Y., Park, J. E., Lee, Y. J., Seo, H. J., Sheen, S. S., Hahn, S., et al. (2013). Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. Journal of Clinical Epidemiology, 66(4), 408-414.
Kim S. Y., Park J. E., Lee Y. J., Seo H. J., Sheen S. S., Hahn S., et al. 2013;Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. Journal of Clinical Epidemiology 66(4):408–414. 10.1016/j.jclinepi.2012.09.016.Kim, S. Y., Park, J. E., Seo, H. J., Lee, Y. J., Jang, B. H., Son, H. J., et al. (2011). NECA's guidance for undertaking systematic reviews and meta-analyses for intervention. Seoul: National Evidence-based Healthcare Collaborating Agency.
Kim S. Y., Park J. E., Seo H. J., Lee Y. J., Jang B. H., Son H. J., et al. 2011;NECA's guidance for undertaking systematic reviews and meta-analyses for intervention Seoul: National Evidence-based Healthcare Collaborating Agency;Klugman, C. M., Peel, J., & Beckmann-Mendez, D. (2011). Art rounds: Teaching interprofessional students visual thinking strategies at one school. Academic Medicine, 86(10), 1266-1271.
Klugman C. M., Peel J., et al, Beckmann-Mendez D.. 2011;Art rounds: Teaching interprofessional students visual thinking strategies at one school. Academic Medicine 86(10):1266–1271. 10.1097/acm.0b013e31822c1427.Lee, Y. H., Ahn, D., Moon, J., & Han, K. (2014). Perception of interprofessional conflicts and interprofessional education by doctors and nurses. Korean Journal of Medical Education, 26(4), 257-264.
Lee Y. H., Ahn D., Moon J., et al, Han K.. 2014;Perception of interprofessional conflicts and interprofessional education by doctors and nurses. Korean Journal of Medical Education 26(4):257–264. 10.3946/kjme.2014.26.4.257.Luctkar-Flude, M., Baker, C., Pulling, C., Mcgraw, R., Dagnone, D., Medves, J., et al. (2010). Evaluating an undergraduate interprofessional simulation-based educational module: Communication, teamwork, and confidence performing cardiac resuscitation skills. Advances in Medical Education and Practice, 1, 59.
Luctkar-Flude M., Baker C., Pulling C., Mcgraw R., Dagnone D., Medves J., et al. 2010;Evaluating an undergraduate interprofessional simulation-based educational module: Communication, teamwork, and confidence performing cardiac resuscitation skills. Advances in Medical Education and Practice 1:59.Martin, J. S., Ummenhofer, W., Manser, T., & Spirig, R. (2010). Interprofessional collaboration among nurses and physicians: Making a difference in patient outcome. The European Journal of Medical Science, 140, w13062.
Martin J. S., Ummenhofer W., Manser T., et al, Spirig R.. 2010;Interprofessional collaboration among nurses and physicians: Making a difference in patient outcome. The European Journal of Medical Science 140:w13062.McGettigan, P., & McKendree, J. (2015). Interprofessional training for final year healthcare students: A mixed methods evaluation of the impact on ward staff and students of a two-week placement and of factors affecting sustainability. BMC Medical Education, 15(1), 185.
McGettigan P., et al, McKendree J.. 2015;Interprofessional training for final year healthcare students: A mixed methods evaluation of the impact on ward staff and students of a two-week placement and of factors affecting sustainability. BMC Medical Education 15(1):185. 10.1186/s12909-015-0436-9.Mohaupt, J., van Soeren, M., Andrusyszyn, M. A., MacMillan, K., Devlin-Cop, S., & Reeves, S. (2012). Understanding interprofessional relationships by the use of contact theory. Journal of Interprofessional Care, 26(5), 370-375.
Mohaupt J., van Soeren M., Andrusyszyn M. A., MacMillan K., Devlin-Cop S., et al, Reeves S.. 2012;Understanding interprofessional relationships by the use of contact theory. Journal of Interprofessional Care 26(5):370–375. 10.3109/13561820.2012.673512.Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264-269.
Moher D., Liberati A., Tetzlaff J., et al, Altman D. G.. 2009;Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine 151(4):264–269. 10.7326/0003-4819-151-4-200908180-00135.Nagelkerk, J., Peterson, T., Pawl, B. L., Teman, S., Anyangu, A. C., Mlynarczyk, S., et al. (2014). Patient safety culture transformation in a children’s hospital: An interprofessional approach. Journal of Interprofessional Care, 28(4), 358-364.
Nagelkerk J., Peterson T., Pawl B. L., Teman S., Anyangu A. C., Mlynarczyk S., et al. 2014;Patient safety culture transformation in a children’s hospital: An interprofessional approach. Journal of Interprofessional Care 28(4):358–364. 10.3109/13561820.2014.885935.Paige, J. T., Garbee, D. D., Kozmenko, V., Yu, Q., Kozmenko, L., Yang, T., et al. (2014). Getting a head start: High-fidelity, simulation-based operating room team training of interprofessional students. Journal of the American College of Surgeons, 218(1), 140-149.
Paige J. T., Garbee D. D., Kozmenko V., Yu Q., Kozmenko L., Yang T., et al. 2014;Getting a head start: High-fidelity, simulation-based operating room team training of interprofessional students. Journal of the American College of Surgeons 218(1):140–149. 10.1016/j.jamcollsurg.2013.09.006.Interprofessional education collaborative expert panel. (2011). Core competencies for interprofessional collaborative practice: Report of an expert panel. Washington, DC: Interprofessional Education Collaborative.
Interprofessional education collaborative expert panel. 2011. Core competencies for interprofessional collaborative practice: Report of an expert panel Washington, DC: Interprofessional Education Collaborative;Parsell, G., & Bligh, J. (1999). The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education, 33(2), 95-100.
Parsell G., et al, Bligh J.. 1999;The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education 33(2):95–100. 10.1046/j.1365-2923.1999.00298.x.Phillips, C. B., Hall, S., & Irving, M. (2016). Impact of interprofessional education about psychological and medical comorbidities on practitioners’ knowledge and collaborative practice: Mixed method evaluation of a national program. BMC Health Services Research, 16(1), 465-474.
Phillips C. B., Hall S., et al, Irving M.. 2016;Impact of interprofessional education about psychological and medical comorbidities on practitioners’ knowledge and collaborative practice: Mixed method evaluation of a national program. BMC Health Services Research 16(1):465–474. 10.1186/s12913-016-1720-z.Vazirani, S., Hays, R. D., Shapiro, M. F., & Cowan, M. (2005). Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. American Journal of Critical Care, 14(1), 71-77.
Vazirani S., Hays R. D., Shapiro M. F., et al, Cowan M.. 2005;Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. American Journal of Critical Care 14(1):71–77.Whelan, J. J., Spencer, J. F., & Rooney, K. (2008). A 'RIPPER' project: Advancing rural inter-professional health education at the university of Tasmania. Rural and Remote Health, 8(1017), 1-9.
Whelan J. J., Spencer J. F., et al, Rooney K.. 2008;A 'RIPPER' project: Advancing rural inter-professional health education at the university of Tasmania. Rural and Remote Health 8(1017):1–9.World Health Organization. (1988). Learning together to work together for health. Report of a WHO study group on multiprofessional education for health personnel: The Team Approach. World Health Organization Technical Report Series, 769, 1-72.
World Health Organization. 1988. Learning together to work together for health. Report of a WHO study group on multiprofessional education for health personnel: The Team Approach. World Health Organization Technical Report Series, 769 1–72.Yoon, B. J., & Lee, J. H. (2010). A review study on interprofessional college education in health care sector, The Journal of Korean Society for School & Community Health Education, 11(1), 149-58.
Yoon B. J., et al, Lee J. H.. 2010;A review study on interprofessional college education in health care sector. The Journal of Korean Society for School & Community Health Education 11(1):149–58.Appendix
